What is the tracheotomy?
Tracheotomy is a surgical tracheal maneuver performed to facilitate breathing when oxygen supply is insufficient.
Specifically, the tracheotomy involves two very important and distinct phases:
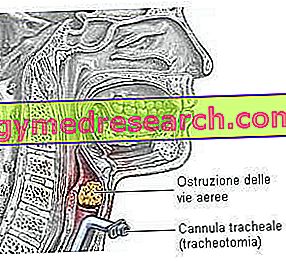
- Temporary dilatation (opening) of the cervical tracheal wall through an incision of the skin at the level of the trachea
- Subsequent placement of a special tracheal cannula able to guarantee the passage of air from the outside towards the lungs and vice versa
Born as an extreme life-saving attempt, the tracheotomy is one of the oldest surgical acts documented up to now, performed essentially to ensure adequate respiration to the patient.
Contrary to what one might imagine, the tracheotomy is today a rather simple operation to be performed for an expert hand; nevertheless, errors during the execution of the maneuver - certainly not rare - can give rise to complications of varying degrees.
However, remember that performing a tracheotomy does not simply mean giving way to a new air passage to optimize breathing: incising the tracheal wall also means altering the respiratory physiology and modulating the cervical anatomy.
Anatomy review to understand ...
The trachea is a flexible and elastic fibrocartilaginous duct very similar to a flattened cylinder in its posterior portion. Its function is to convey the air from the outside towards the bronchi and lungs (inspiratory phase) and vice versa (expiratory phase).
The trachea is a connection structure between the larynx and the bronchi:
- At the upper extremity, the trachea originates from the cricoid cartilage of the larynx (at the level of the sixth cervical vertebra)
- At the lower end, the trachea ends at the thoracic level dividing into the two primary bronchi (at the level of the fifth thoracic vertebra)
The trachea consists of 15-20 cartilage rings superimposed on each other, connected to each other by connective tissue. The tracheotomy can be performed between the second and fourth tracheal rings, thus positioned immediately below the cricoid cartilage.
Tracheotomy or tracheostomy?
Before going into the treatment of the surgical act, it is good to distinguish two terms that are often mistaken for synonyms.
- Tracheotomy: temporary opening of the trachea (after removal of the cannula, the hole created - called the tracheal stoma - closes spontaneously, thus restoring natural breathing)
- Tracheostomy: permanent opening of the trachea. It is performed by connecting the tracheal breccia (ie the gap created) to the edges of the skin where the incision was made: in this way, the tracheal lumen is directly connected with the external environment.
Why is it performed?
The tracheotomy can be performed on all occasions when the air cannot reach the lungs in sufficient quantity.
The intervention can be carried out both in urgent and non-urgent conditions (for further information, read "types of tracheotomy"):
- Presence of mucus or other secretions in the trachea (a phenomenon linked in particular to swallowing difficulties)
- Upper airway obstruction due to facial trauma, infections, stenosis (narrowing), angioedema
- Airway obstruction due to paralysis of the throat muscles or neoplasms
- Need for continuous ventilation in patients with chronic respiratory failure
- Severe obstructive sleep apnea in patients intolerant to the so-called CPAP ( Continuous Positive Airway Pressure, which consists in the use of positive pressure regulators)
- Prevention of bronchial obstruction induced by respiratory failure
- Severe burns of the oral cavity
- Chronic stenoses of the larynx and trachea
- Prevention of aspiration of gastric contents
- Other situations that make endotracheal intubation impractical


