What is the Crystalline
The crystalline lens is a biconvex lens located inside the eyeball, between the iris and the vitreous body.
This structure is one of the main components of the dioptric apparatus of the eye: thanks to the action of the ciliary muscle, the crystalline lens is able to modify its shape to "automatically" adjust the focusing of light rays on the retina, based on the proximity or less than the object to be displayed (refractive power variation). This ability is physiologically reduced with age, when presbyopia occurs. The crystalline lens also meets changes in thickness, elasticity and transparency.

Relations with other structures
The crystalline lens is placed in the anterior area of the eyeball, just behind the "diaphragm" formed by the iris .
The lens is kept in its natural seat by a restraining apparatus, called Zinn's zonula, consisting of thin tendons of connective tissue (zonular fibers), which anchor it to the ciliary body . Furthermore, the accommodation process depends on the action of these structures. This apparatus, therefore, allows to vary the refractive power of the crystalline lens, modifying its shape, to allow the focusing of the images observed on the retina.
The crystalline lens and the ciliary body separate the eye into two parts: forward, facing the anterior chamber in which the aqueous humor is present and, posteriorly, limit the vitreous chamber containing a gelatinous substance ( vitreous humor ) which helps to maintain the spherical structure of the eyeball.
The crystalline lens has neither nerves nor blood or lymphatic vessels. Indeed, the presence of these structures would obstruct the passage of light. Being avascular, the structure takes the nutrients it needs from the aqueous humor.
Features and properties
The crystalline lens is a perfectly transparent structure, formed by concentric layers of cells arranged in an orderly manner, and covered by a capsule of fibrous and elastic connective tissue. This biconvex-shaped lens has a diameter of about 10 mm and an axial thickness of 3-4.5 mm. In relation to its shape, two faces are considered: one anterior and one posterior. The circular contour of the crystalline is called, instead, equator and represents the contact angle between the two faces. The equatorial circumference is 0.5-1 mm from the ciliary processes and has slight indentations, which depend on the action of the fibers of the zonula.
The front face of the crystalline lens is less convex than the back face (the front curvature radius is 10 mm, while the rear one is 6 mm). Both are, however, more inflected in the child and less in the elderly. Furthermore, the curvature of the faces changes in the eye at rest and in the distance or near vision: the crystalline lens is a flexible lens, able to vary its shape, and therefore its dioptric power, to adjust the focus.
From the vertex of the cornea, the anterior pole of the lens (ie the central point of the anterior aspect) is about 3.5 mm, while the posterior pole is located approximately 16 mm from the central fovea of the retina.
Structure
Structurally, the crystalline lens is composed of three elements:
- Capsule (or crystalloid) : extremely thin, flexible and transparent membrane, which completely covers the lens. Under the electron microscope, the capsule has a continuous lamellar structure of homogeneous appearance, consisting of numerous elastic fibers. These, even in the absence of an external force, contract, making the lens spherical. At the equator, the capsular fibers join up with those of the suspensory ligaments in the Zinn zonula. The integrity of the capsule is essential for metabolic exchanges and the maintenance of transparency, an essential property of the crystalline lens so that light rays can easily pass through it and are correctly projected to the retinal level.
- Subcapsular epithelium : covers the inner surface of the capsule in its anterior and equatorial tract.
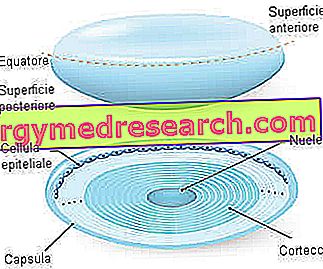
- Parenchyma : it is the substance of the crystalline lens, consisting of prismatic cells in the form of an arched ribbon (called crystalline fibers), arranged in concentric lamellae cemented by glycoproteins. The transparency of the crystalline lens depends on the fact that these fibers are tightly pressed together. In the parenchyma, an inner and central portion (nucleus) and a superficial portion (cortical layer) can be distinguished.

Functions
Together with the cornea, the lens converges the light waves that penetrate the eye. In this way, the image projected at the retinal level will be in focus.
The task of the lens consists, in particular, in varying the focal distance of the optical system, changing its shape, therefore its refractive power, to adapt it to the distance of the observed image and make its vision clear. To see objects from very close, for example, the lens must become more convex to increase its refractive power.
In addition to the dioptric function and accommodation, the lens absorbs some of the ultraviolet rays, thus contributing to the protection of the retina.
Accomodation
The ability of the lens to modify the power of refraction in near and far vision is called accommodation .
In order to clearly observe an object, the light reflected from each of its points must converge in a single point of the retina. When looking at a distant object, the light rays that reach the lens are almost parallel to each other and the refractive power needed to focus the images on the retina must be low. The crystalline lens must therefore be relatively flattened (weaker lens).
In contrast, the light waves reflected by a nearby object diverge when they reach the eye; in this case, a rounder lens is needed to increase the refractive power and make the rays converge on the retina.
How the shape of the lens is modified
The shape of the crystalline lens is controlled by the ciliary muscle, using the tension it exerts on the zonular fibers.
- At rest, the tension exerted by the suspensory ligaments in the Zinn zonula exceeds the intrinsic elastic resistance of the capsule and bends the lens, making it flattened in shape. In this position, the eye focuses on distant images.
- When the ciliary muscle contracts, however, the ciliary body moves towards the lens, the tension of the suspensory ligaments is reduced and the crystalline takes on an almost spherical shape. In this position, the eye focuses on nearby images.
The accommodation is under the control of the parasympathetic autonomic nervous system that activates the contraction of the ciliary muscle for near vision. In the absence of parasympathetic activity, the ciliary muscle is released.
Defects of vision
The normal eye ( emmetrope ) sees well both distant objects and neighboring ones.
If the light rays reflected by an object are not properly focused on the retina, however, the vision is distorted. Many causes can produce this effect, some of which depend on the crystalline lens.
Myopia and hypermetropia
In myopia and hypermetropia, there is a discrepancy between the curvature of the lens (or cornea) and the length of the eyeball, and therefore the distance from the retina.
In myopia, a person can clearly see objects closely, but not distant ones, since the dioptric power of the crystalline (or cornea) is too powerful for eye length. In other words, near objects are brought into focus without accommodation, while distant objects are focused on a plane anterior to the retina.
In hypermetropia, on the other hand, distant images are focused without accommodation and the neighboring ones are focused on a posterior plane to the retina (the hypermetropic eye is a "shorter" eye than normal).
Astigmatism
In astigmatism, irregularities on the surface of the cornea or lens produce uneven refraction of the observed images. Therefore, the light waves instead of converging on the retina in the same focal point, are differently focused in the various transverse planes. This results in less visual clarity.

Presbyopia
Over the years, the lens loses its elasticity, becoming more rigid and resistant to changes in shape. The result is a gradual reduction in accommodation and greater dependence on reading glasses for near vision.
Crystalline diseases
The pathological processes affecting the lens are divided into:
- Transparency anomalies;
- Form anomalies;
- Position anomalies.
Cataract
Cataract is a disease characterized by the progressive and constant opacification of the lens.
This alteration is usually related to age (senile cataract), but the causes can be multiple. In fact, there are also congenital forms (already present at birth) due to genetic factors, infectious processes (eg rubella and toxoplasmosis contracted during pregnancy), metabolic disorders of the mother and exposure to radiation.

The most important symptom of cataract is, therefore, the loss of sight (usually within months or years); other manifestations are the easy glare, the less vivid color perception and the sensation of blurring or doubling of the images. Cataracts can be treated with corrective eye surgery.
Ectopia lentis or subluxation
Ectopopia lentis is a poor positioning of the crystalline lens compared to its normal site. The displacement may be partial (subluxation) or complete (dislocation / dislocation).
The crystalline lens, being no longer perfectly anchored, moves back and forth, creating serious visual disturbances. Lentis ectopia can be congenital or caused by a traumatic or metabolic alteration (eg enzyme deficiencies that compromise the organization of the zonular fibers). Furthermore, it can be found in the field of anterior uveal tumors, chronic cyclite, macrophthalmos, syphilis, homocystinuria and Marfan syndrome.
The subluxation of the crystalline lens is highlighted by the presence of iridodonesi (flickering of the iris) and facodonesi (trembling of the crystalline). Possible consequence is glaucoma.
Lenticono and other anomalies
The lenticono is a malformation which consists in the oval or circular protrusion of the anterior or posterior pole of the crystalline lens, which alters its normal curvature (to make a comparison, the pathological process is similar to the keratoconus of the cornea).
In general, this conical deformation is congenital and may or may not be associated with systemic diseases, such as spina bifida and Alport syndrome (a condition also characterized by renal alterations, often with hematuria and variable degree hypoacusis).
The lenticono causes astigmatic type of refraction disorders that are difficult to correct. Sometimes, opacity of the crystalline lens, strabismus and retinoblastoma can also be found. In more serious cases, surgical therapy, with the removal of the lens and its replacement with a synthetic lens, can improve eyesight.
Other shape anomalies that more rarely affect the crystalline lens include microsphere (small and spherical crystalline), microfachia (smaller than normal diameter), spherophakia and coloboma.


