Generality
Syringomyelia is a neurological disease characterized by the formation of fluid-filled cysts in the spinal cord.
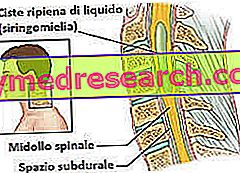
Figure: syringomyelia.
From the site: mdguidelines.com
In the long run, the presence of these cysts, called syringes, creates damage to the spinal cord; thus appear various disorders, such as pain in several points of the body, sense of stiffness and weakness, muscular atrophy, loss of reflexes, spasms in the legs, etc.
Syringomyelia may be due to different causes; in most cases, it is associated with a malformation of the cerebellum known as the Chiari malformation.
For a correct diagnosis, an accurate physical examination of the patient, an analysis of his clinical history and some diagnostic imaging tests are required.
The only way to empty the syringes and solve (at least in part) the symptoms involves resorting to surgery.
What is syringomyelia?
Syringomyelia is a rare pathological condition, following which one or more cysts filled with fluid form inside the spinal canal.
If the cysts (also called syringes or fistulas ) expand, they can severely damage the spinal cord and affect the transmission of nerve signals.
WHAT ARE THE CYSTS AND WHAT DO THEY CONTAIN?
Syringes are ducts or cavities (in Greek, " syrinx " means "duct") containing cerebrospinal fluid (or liquor ).

Figure: the three meninges that surround the central nervous system.
The meninges are protective membranes: the outermost is the dura mater; the central is the arachnoid; finally, the innermost is the pious mother.
The subarachnoid space, between arachnoid and pia mater, contains the cephalorachidian fluid.
The liquor is a colorless fluid that surrounds the central nervous system (or CNS ), protects it from any trauma, provides it with nourishment and regulates internal pressure (intracranial pressure).
The cerebrospinal fluid is produced inside the cerebral ventricles, precisely at the level of the choroid plexuses; from here, it flows into the subarachnoid space, or the interposed area between the meninga pia mater and the meninge arachnoid.
Epidemiology
According to some statistical studies, syringomyelia would have a prevalence of about 8 cases per 100, 000 people. Usually, the appearance of its characteristic symptoms occurs between the ages of 25 and 40 and its evolution is generally slow.
Many patients with syringomyelia are also affected by a structural alteration of the cerebellum, known as the Chiari malformation (or Arnold-Chiari or Arnold-Chiari syndrome ).
Causes
Syringomyelia can be a congenital condition, that is present since birth, or acquired, that is, it arose during the course of a life following a particular event or in association with a specific morbid condition.
CONGENITAL SYRINGOMYELY
Congenital forms of syringomyelia are due to Arnold-Chiari syndrome.
Arnold-Chiari syndrome is a cerebellar malformation (that is, the cerebellum) characterized by a downward movement, precisely in the direction of the occipital hole and the spinal canal, of the basal portion of the cerebellum.

In other words, it is a cerebellar hernia, in which part of the cerebellum protrudes from the occipital hole invading the canal containing the spinal cord.
ACQUIRED SYRINGOMYELY
The main causes that can lead to the establishment of an acquired syringomyelia are:
- A spinal cord trauma . Among the various traumas that can lead to syringomyelia there is the fracture of the vertebrae.
- A meningitis . Meningitis is the inflammation of the membranes surrounding the central nervous system (NB: the CNS is composed of encephalon and spinal cord). At the origin of meningitis there may be a viral or bacterial infection.
Arachnoiditis, the inflammation of the arachnoid, is the most common form of meningitis that can give syringomyelia.
- A spinal cord tumor . According to experts, the presence of a tumor mass within the spinal canal would prevent the normal circulation of the liquor, thus giving rise to a localized collection, then to a syringe.
- Rigid column syndrome . It is a particular neurological disease, characterized by adhesions between the spinal cord and the vertebral column; adhesions that prevent the marrow from flowing normally.
The typical symptoms and signs of rigid spine syndrome are: leg pain, back pain, scoliosis, urinary incontinence or retention, muscle weakness and numbness, etc.
- A hemorrhage within the spinal cord (or hematomyelia ). Hematomyelia can be spontaneous or traumatic and usually affects the arterial vessels of the gray substance. Usually, the traumas that can give rise to hematomyelia are blows to the vertebrae.
Readers are reminded that some forms of syringomyelia arise without a precise cause or a decipherable reason. In such situations, one speaks of acquired idiopathic syringomyelia .
POINTS IN SUSPENSION
Doctors and researchers are still trying to solve some questions related to the formation of syringes, and how these damage the spinal cord.
According to some theories, it appears that syringes originate from an obstruction to the CSF flow in the subarachnoid space and that damage to the spinal cord is the result of pressure exerted by the cysts on the marrow itself.
Symptoms and Complications
To learn more: Symptoms Syringomyelia
The classic signs and symptoms of syringomyelia are:
- Weakness and muscular atrophy
- Loss of reflexes
- Loss of sensitivity to pain and environmental temperature (NB: in other words, the skin fails to feel the sensation of intense heat or icy cold)
- Stiffness in the back, shoulders, arms and legs
- Pain in the neck, arms, hands and back
- Intestinal and bladder problems. The patient loses control of the anal and bladder sphincters.
- Extreme muscle weakness and spasms in the legs
- Pain and numbness in the face
These manifestations, which at the onset are generally not very marked, are the result of the damage that the syringes produce to the spinal cord.
CONGENITAL SYRINGOMYELY
Despite being present from birth, congenital syringes tend to cause the first symptoms in adulthood. The reason for this is explained by the fact that cysts take some time to produce significant damage to the spinal cord.
In addition to being affected by Chiari malformation, patients with congenital syringomyelia may also suffer from hydrocephalus and arachnoiditis.
What is hydrocephalus?
The term hydrocephalus indicates a serious disease due to an abnormal increase in the cerebrospinal fluid contained in the subarachnoid space and in the cerebral ventricles.
This enormous increase in CSF occurs when, previously, intracranial pressure ( intracranial hypertension ) is increased. The cause of hydrocephalus can be: a brain tumor, a cerebral hemorrhage, a meningitis, an encephalitis, CNS malformations and so on.
The main signs of hydrocephalus are: increased head circumference, neck pain, epilepsy and convulsions.
ACQUIRED SYRINGOMYELY
From the event that triggers the formation of syringes to the onset of the first symptoms, months or years can also pass. Therefore, similar to what happens for congenital syringomyelia, damage to the spinal cord has a very slow progression.
Generally, when at the origin there is a trauma (post-traumatic syringomyelia), the signs of the disease appear on one side only of the body.
WHEN TO REFER TO THE DOCTOR?
In the presence of one or more of the aforementioned symptoms, it is advisable to contact your doctor immediately to arrange an in-depth examination to identify the causes of the disorders.
The evaluation of an expert is decisive, since syringomyelia is generally the result of other pre-existing diseases (which require an appropriate treatment).
If you have been a victim of severe back trauma, you may not initially experience any disorder related to syringomyelia. However, this could still develop after a certain period and become symptomatic even after several months or years. Therefore, if ever suspicious symptoms appear, it is advisable to contact your doctor and tell him about the traumatic event you have suffered.
COMPLICATIONS
Syringomyelia is a potentially degenerative disease, as the syringes can widen, damage the spinal cord more and more and alter the patient's nervous functions even more important.
Some classic expressions of such complications are:
- Scoliosis . It is an abnormal curvature of the spine.
- Widespread chronic pain . The greater the damage to the spinal cord, the more intense and persistent the painful sensation in the neck, arms, hands and back becomes.
- Serious motor difficulties . If atrophy and muscle weakness get worse, the patient can have serious problems even walking.
Diagnosis
To diagnose syringomyelia, the first step is the physical examination and the analysis of clinical history.
Therefore, once these two preliminary checks have been performed, diagnostic imaging texts, such as nuclear magnetic resonance (NMR), the TAC, become of fundamental importance; for some patients, a lumbar puncture is also required.
EXAMINATION OBJECTIVE
During the physical examination, the doctor evaluates the symptomatological situation, asking the patient to describe in detail the disturbed sensations.
EXAMINATION OF CLINICAL HISTORY
When a doctor analyzes the medical history of a patient, he goes in search of the possible triggering factors and of any situations predisposing the disease. For example, they are being investigated:
- Pathologies suffered in the past by the patient
- The pathologies in place at the time of the examination
- Recurrent diseases within the family to which the patient belongs (a family member with similar disorders, etc.)
- Situations that have seen the patient be the victim of spinal cord trauma.

Figure: Syringomyelia at nuclear magnetic resonance. The syringe is circled in red.
NUCLEAR MAGNETIC RESONANCE (RMN)
There are two different types of nuclear magnetic resonance ( NMR ):
- Classical magnetic resonance . Thanks to the creation of magnetic fields, the MRI provides a detailed image of the spinal cord, without exposing the patient to harmful ionizing radiation.
- Magnetic resonance with contrast medium . The instrument used is the same used for classical NMR. The only difference is that a contrast liquid is injected into the patient, which serves to reveal the presence of any spinal cord tumors or other similar abnormalities.
The contrast liquid represents the only contraindication of the examination: this in fact could have toxic effects or trigger an allergy.
TAC (COMPUTERIZED AXIAL TOMOGRAPHY)
Computerized axial tomography ( CT ) provides clear images of the internal organs, including the spinal cord. During its execution, the subject is exposed to a minimum amount of harmful ionizing radiation; therefore the test is to be considered, albeit minimally, invasive.
LUMBAR PUNCTURE
The lumbar puncture consists in taking a sample of cerebrospinal fluid and in its analysis in the laboratory. To remove the liquor, a needle inserted between the lumbar vertebrae L3-L4 or L4-L5 is used.
The lumbar puncture is of considerable utility to investigate the causes of syringomyelia: in fact, it can detect possible infections at the level of the meninges.
Treatment
When the symptoms of syringomyelia interfere with normal daily life, the only remedy is surgery.
On the contrary, when the syringomyelia does not cause any disturbance, the situation is simply monitored (principle of surveillance).
PRINCIPLE OF MONITORING
The principle of surveillance consists in subjecting the patient to periodic magnetic resonances and to neurological control examinations. This approach is indicated for subjects with asymptomatic syringes (ie that do not cause any obvious symptoms).
Although it is a very remote hypothesis, it is possible that the cysts vanish spontaneously.
SURGERY
The surgical procedure to be adopted is chosen based on the conditions that caused (or accompany) syringomyelia. Therefore:
- In the case of Chiari malformation, the operating surgeon can use the following operations: decompression of the posterior fossa, decompression of the spinal cord ( decompressive laminectomy ) and decompressive incision of the dura mater . All three procedures aim to reduce compression against the cerebellum and spinal cord, trying to increase the space available to them. More available space means an improvement in the liquor flow, therefore a possible emptying of the syringes.
With the decompression of the posterior fossa, part of the posterior portion of the occipital bone is removed.
With the decompressive laminectomy, the vertebral portion delimiting the hole within which the spinal cord passes passes.
Finally, with the decompressive incision of the dura mater, the most external meningis is incised.
- In the case of spinal cord cancer, the surgeon eliminates the tumor mass in such a way as to restore the flow of liquor. After removal, the syringe empties automatically, causing the symptoms that characterized it to revert before surgery.
- In case of rigid spine syndrome, the surgeon can use various methods. The main one consists in "dissolving" the adhesions that block the column to the spinal cord.
Possible complications of the syringoperitoneal shunt:
- Spinal cord injury
- Infections
- Blocks to the circulation of the fluid
- Hemorrhages within the spinal cord (hematomyelia)
Alongside these specific surgical techniques, there is also a procedure aimed at temporarily reducing symptoms and pain (palliative therapy), known as a surgical shunt .
The surgical shunt is a drainage system, consisting of a flexible tube that allows the emptying of the syringes. In general, the excess fluid is drained into the abdomen ( syringoperitoneal shunt ), in a similar way to what is done in case of hydrocephalus ( ventriculoperitoneal shunt ).
Since this is a rather delicate method and not without complications, before putting it into practice the doctor carefully assesses the situation and discusses possible risks with the patient.
Who performs surgery?
The operating surgeon is a doctor specializing in neurosurgery, which is the branch of surgery that deals specifically with problems and diseases of the central and peripheral nervous system.
CARE IN CASE OF RECIDIVA
Even when properly treated, syringomyelia can recur after some time (recurrence).
To promptly notice a possible relapse, it is advisable to periodically undergo appropriate medical checks and a nuclear magnetic resonance of the back.
The reformation of one or more syringes requires a second surgical procedure, often a cyst drainage, the benefits of which could only be temporary.
SOME ADVICES
Syringomyelia could strongly affect the quality of life of the affected person and any of his daily activities. Therefore, it is good practice:
- Avoid lifting weights, making efforts and "loading" your back, as these are three actions that can worsen the symptoms, especially pain.
- Contact a good physiotherapist. Thanks to appropriate physiotherapy, it is possible to improve mobility, strengthen the muscles and better endure the efforts.
- Treat chronic pain with appropriate medications. If the pain is chronic and tormenting, it is good for the patient to ask his doctor to plan an adequate pain relief.
- Seek comfort from loved ones (friends or relatives) and join a support group for people with syringomyelia. They are two different ways of improving the mood, often depressed due to the limitations imposed by the disease.
Prognosis
The prognosis depends on the severity of the causes that triggered the syringomyelia and the effectiveness of the surgery.
- It depends on the severity of the triggers because, the more serious the condition that triggers syringomyelia, the more likely it is that the consequences of the disease are permanent.
- It depends on the effectiveness of the treatment since medical intervention does not always restore the normal flow of CSF, as it does not always allow the definitive elimination of cysts associated with syringomyelia.