Generality
Rectal cancer, or rectal tumor, is a malignant neoplasm of the large intestine, resulting from the uncontrolled proliferation of a cell of the rectum wall.

The typical symptoms of rectal cancer consist of: rectal bleeding, blood in the stool, anemia, abdominal pain, abdominal cramps, diarrhea, constipation, a sense of incomplete bowel emptying after defecation and a sense of foreign body in the rectum.
An accurate diagnosis of rectal cancer is based on flexible sigmoidoscopy and tumor biopsy.
Possible treatments are: surgical therapy, radiotherapy, chemotherapy and so-called "targeted therapy".
Brief anatomical review of the rectum?
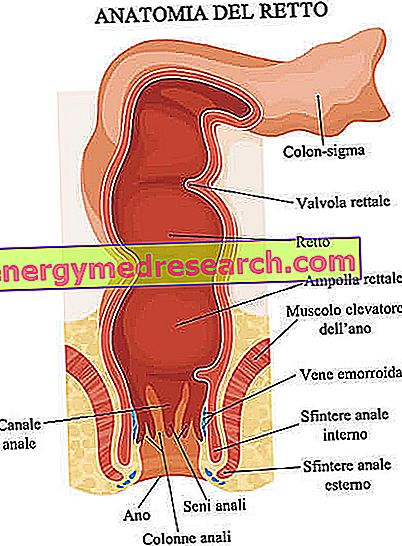
The rectum is the terminal section of the large intestine or large intestine .
Generally between 12 and 15 centimeters long, and beginning between the II and III sacral vertebrae, the rectum follows the intestinal tract called sigma or colon-sigma and precedes the anus .
Normally, anatomists divide the rectum into two portions: an upper portion, called the pelvic portion, in which the so-called ampulla resides, and a lower portion, called the anal portion, which consists substantially in the so-called anal canal .
Thanks to a histological composition similar to that of the rest of the large intestine, the rectum contributes to the function it covers: absorbing water and electrolytes (sodium, potassium, chlorine, etc.) from the digested food.
Moreover, being the terminal section of the intestine, it also covers the important task of receiving the faeces and favoring their expulsion through the anus ( defecation ).
What is rectal cancer?
Rectal cancer, or rectal tumor, is the malignant neoplasm of the large intestine resulting from the uncontrolled proliferation of one of the cells present in the wall of the rectum.
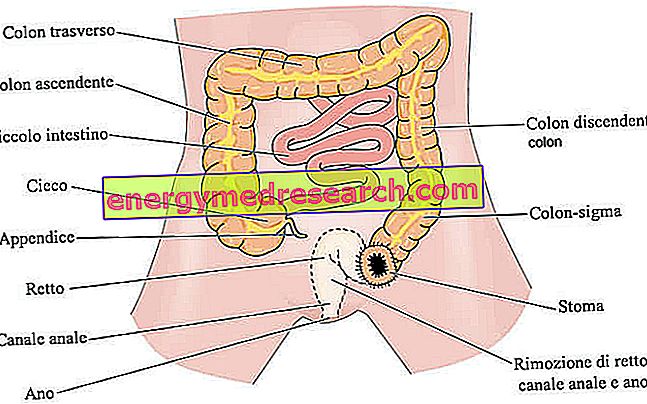
Because of the histological and functional similarity of the rectum with the remaining parts of the large intestine, this tumor belongs to the group of malignant neoplasms of the colon-rectum, a group that includes: the ascending colon tumor, the transverse colon tumor, the descending colon tumor and sigmoid (or colon-sigma ) tumor .
Curiosity
Among colorectal neoplasms, rectal cancer is the most common (50% of clinical cases), followed by: sigmoid tumor (19-21% of cases), ascending colon cancer (16% of cases ), transverse colon cancer (8% of cases) and descending colon cancer (6% of cases).
Types of rectal cancer
Rectal cancer is almost always an adenocarcinoma, ie a malignant tumor that originates from the epithelial cells of the intestinal mucosa .
In the large intestine, epithelial cells with these properties constitute the so-called mucous membrane, that is the innermost layer of the intestinal wall, the one that takes direct contact with the food during digestion.
In those rare circumstances in which it is not an adenocarcinoma, rectal cancer can be:
- A non-Hodgkin's lymphoma of the genus MALToma ;
- A squamous carcinoma ;
- A gastrointestinal stromal tumor ;
- A leiomyosarcoma ;
- A carcinoid .
Causes
Like many other malignant tumors, rectal cancer is also the result of a slow accumulation of genetic mutations by one of the cells of the rectal intestinal wall.
Despite numerous research on this, doctors have not yet identified the precise causes of these mutations; however they are quite sure of the risk factors of the disease in question.
What are the risk factors for rectal cancer?
Going into details, the risk factors for rectal cancer certainly include:
- The presence of hereditary conditions associated with the development of benign or malignant tumors along the gastrointestinal tract (eg: Lynch II syndrome and familial adenomatous polyposis );
- Some familiarity with rectal cancer or similar tumors (eg, colon cancer);
- An unhealthy diet, in which the consumption of red meats, fatty foods of animal origin and fried foods prevails, and in which food fibers and the supply of fresh fruits and vegetables are scarce;
- The presence in the rectum of adenomatous polyps ;
- Inflammatory bowel diseases (eg: Crohn's disease or ulcerative colitis );
- Advanced age;
- Obesity, cigarette smoking, a sedentary lifestyle and alcohol consumption;
- Belonging to the African-American race;
Brief reminder of epidemiology
Globally, rectal cancer and other neoplasms of the large intestine affect, independently, more than one million people every year and represent, as a whole, the second most common form of cancer, among women, and the third most common form of cancer among men.
Symptoms and complications
Fruit of the intestinal obstruction produced by the growing tumor mass and the infiltration of the latter along the intestinal wall, with consequent vascular damage, the classic symptoms and signs of rectal cancer consist of:
- Internal bleeding phenomena, which involve the more or less evident presence of blood in the stool;
- Rectal bleeding;
- Anemia due to excessive blood loss;
- Fatigue, fatigue, dyspnea at rest and unexplained weight loss. They are all symptoms consequent to the anemic state;
- Diarrhea alternating with constipation;
- Production of ribbon-shaped stools;
- Sense of incomplete bowel emptying after defecation;
- Pain in the rectal area;
- Cramps in the lower abdomen;
- Burning and anal itching;
- Sense of foreign body at rectal level.
Complications
Like most cancers, rectal cancer has an infiltrative power, which allows it, at an advanced stage of the disease, to invade anatomically adjacent organs and lymph nodes, in addition to disseminating metastasis (through the blood and lymph) ie cancer cells) in anatomically distant organs and lymph nodes.
Among the organs most affected by metastases from rectal cancer are the liver, lungs, bones and brain .
Diagnosis
In general, the diagnostic procedure for the detection of rectal cancer starts from the physical examination and from the anamnesis; then, he proceeds with a series of laboratory tests on blood and feces, and with a digital rectal exploration; finally, it ends with some instrumental tests - among these, flexible rectosigmoidoscopy and colonoscopy are the most important - and a tumor biopsy.
Other useful instrumental tests:
- Barium sulphate base enema
- Trans-rectal endoscopic ultrasound
- CT scan of the chest and abdominal-pelvic region
Importance of biopsy
Tumor biopsy is the only diagnostic test that allows to establish, with absolute certainty, the type of tumor in the present rectum and the stage of progress (or staging ) of the latter.
For treating physicians, knowledge of staging a tumor is essential for planning the most appropriate therapy.
STAGING OF THE TUMOR IN THE ADENOCARCINOMA TYPE
According to the so-called Dukes classification, the possible stages of advancement of an adenocarcinoma of the rectum are four in total: stage A, stage B, stage C and stage D.
- Stage A: this is the least serious stage.
At this stage, the tumor resides almost exclusively on the mucous membrane of the intestine; rarely, it goes into the layers below the mucosa.
It never affects the lymph nodes;
- Stage B: this is the stage of gravity immediately following stage A.
At this stage, the tumor mass has penetrated beyond the intestinal mucosa and affects the underlying muscle layer.
Even in such circumstances it never involves any lymph nodes.
- Stage C: on a scale of increasing gravity, it ranks third.
At this stage, the tumor has gone beyond the muscular layer, invading the outermost layer of the intestinal wall and the first regional lymph nodes.
- Stage D: is the most serious stage.
At this stage, the tumor has affected most of the regional lymph nodes and disseminated metastases in various organs of the body.
Therapy
Currently, rectal cancer patients can count on at least 4 different types of treatment: surgical therapy, radiation therapy, chemotherapy and so-called " targeted therapy ".
The ways in which doctors practice these types of treatment and combine them, to obtain the best results, depend mainly on the stage of progress of the neoplasm and, secondly, on the precise location of the tumor mass and the state of health of the patient.
Is rectal cancer curable?
Rectal cancer is treatable with a good success rate as long as its extension is limited to the intestinal wall (neoplasms in stages A and B).
In fact, as it expands elsewhere, it becomes progressively less and less possible to be eradicated and impossible to eradicate (most cases of cancer in stage C and stage D tumors).
The expansion of the tumor in sites other than that of origin inevitably also changes the purpose of the therapy: if for early stage neoplasms the therapeutic purpose is to achieve healing, for neoplasms at more advanced stages, the purpose of treatments it is symptomatic-palliative, as the chances of recovery are minimized.
Surgical therapy
Surgical therapy is essential to achieve recovery from cancer at the rectum in the early stages.
It includes several approaches, including:
- Trans-anal excision . It is indicated for the removal of stage A and tumors limited to the intestinal mucosa. Access to the tumor mass occurs through the anus.
- Mesorectal excision . It is indicated for the removal of rectal tumors that have penetrated beyond the mucous membrane. Performed by laparoscopy, it involves the removal of the part of the rectum carrying the neoplasm and the removal of the mesorectum.
After its realization, it requires the execution of an abdominal stoma (colostomy or rectostomy), for the expulsion of the faeces.
- Low anterior resection with anastomosis . It is indicated for the removal of at least stage B rectal tumors located in the upper part of the rectum. It involves the removal of the rectum section with the neoplasm and, if necessary, of the contaminated regional lymph nodes.
The anastomosis serves to connect the healthy intestine segments, in order to restore the continuity of the digestive system.
- Abdominal-perineal resection . It is indicated for the removal of at least stage B rectal tumors located near the anus. It involves the removal of the stretch of the rectum bearing the tumor mass and, if necessary, the contaminated regional lymph nodes.
After its completion, the surgeon must perform an abdominal stoma (colostomy or rectostomy), in order to guarantee a passage for the expulsion of the faeces.
- Pelvic exentation . It is the surgical procedure of removal of the pelvic organs (colon, descendant, rectum, anus, bladder, urethra, prostate in man, and ovaries, cervix and vagina in women).
It is applied when the rectal neoplasm is at an advanced stage and has contaminated the organs close to the large intestine.
It is more like a symptomatic palliative treatment.
- Bypass obstructive tumors . It is a procedure that serves to circumvent the blockage at the passage of the stools, deriving from the presence of the tumor mass within the rectum.
It is used in the presence of rectal tumors at an advanced stage and surgical removal is impractical.
Radiotherapy and chemotherapy
Radiation therapy involves exposing a tumor mass to a certain dose of high-energy ionizing radiation, with the aim of destroying the neoplastic cells.
Chemotherapy, on the other hand, consists of the administration, intravenously or orally, of drugs capable of killing rapidly growing cells, including tumor cells.
In the presence of rectal cancer, radiotherapy and chemotherapy can be used as:
- Pre-surgical treatments (or neoadjuvants ), to reduce the size of the tumor mass in order to facilitate its subsequent removal.
- Post-surgical (or adjuvant ) treatments, to destroy cancer cells that may have survived after surgical therapy.
- Symptomatic-palliative treatments, when, due to the dissemination of metastases in various parts of the body, an effective removal of the tumor is impractical.
Targeted therapy
The " targeted therapy " is a treatment based on particular drugs (eg: bevacizumab, ramucirumab, cetuximab, panitumumab, regorafenib etc.), which specifically counteract everything that promotes the growth and development of cancer cells.
In the treatment of rectal cancer, "targeted therapy" is used as a symptomatic remedy for advanced neoplasms.
Prognosis
Prognosis of rectal cancer depends closely on the stage of neoplasia. In fact, several medical studies report that:
- For stage A tumors, the 5-year survival rate from diagnosis is at least 80%;
- For stage B tumors, the 5-year survival rate from diagnosis is between 50 and 60%;
- For stage C tumors, the 5-year survival rate from the diagnosis is 30-40%;
- Finally, for stage D tumors, the 5-year survival rate from diagnosis is less than 10%.
Prevention
According to the doctors, to reduce the likelihood of developing rectal cancer it is good to limit the modifiable risk factors (incorrect diet, sedentary lifestyle, obesity, etc.).


