Generality
In vitro fertilization ( IVF or IVF ) is a procedure developed by the Englishman Robert Edwards, thanks to which - in 1978 - Louise Brown was born, the result of his studies and the first human being conceived in a test tube.
The technique is based on the collection of oocytes by vaginal way and on their subsequent fertilization in the laboratory, using the sperm of the partner or an anonymous donor. Similarly, if the female germ cells are unsuitable for generation, the oocytes from a donor external to the couple can be used.
Once fertilization has taken place, one to three embryos are simultaneously transferred to the woman's uterus, a natural site for their development.
When to use
In vitro fertilization is traditionally used in cases of tubal alteration and obstruction (tubal sterility) or their congenital or acquired deficiency (eg due to surgical removal).
As seen in the article dedicated to female infertility, all these conditions prevent or make the meeting of the egg cell with spermatozoa very difficult. The union of gametes is then carried out in the laboratory bypassing the organic impediment.
To consider also the possibility of giving a pregnancy to women who have had their ovaries removed, to those who are missing from birth and in all cases of ovarian failure. Lacking this essential organ for female hormonal regulation, it is necessary not only to resort to oocytes donated by another woman, but also to guarantee the implantation and progression of pregnancy through the association of appropriate hormone replacement therapy.
The same technique can be used in the presence of endometriosis, poor sperm vitality or when artificial insemination fails.
How to do it
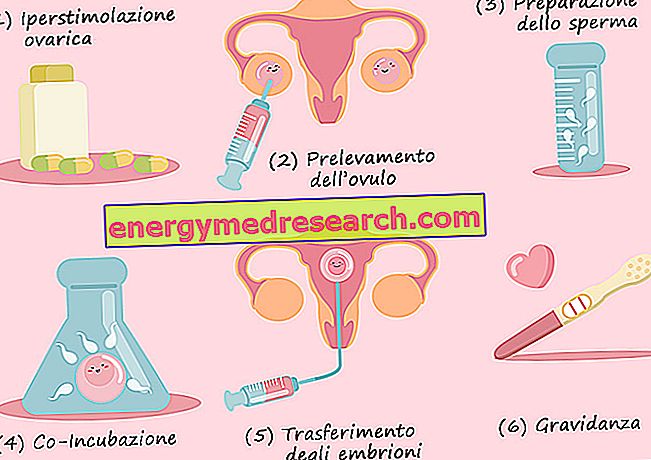
First of all, women's ovulation is controlled by hormonal stimulation, with the aim of producing multiple ovulation. The need to collect more eggs derives from a simple consideration: how many more embryos are transferred to the uterus and the greater the possibilities of implantation.
The oocytes are taken under ultrasound guidance, mostly under general anesthesia, selected and incubated at 37 degrees, for 24-48 hours, in prepared liquids and with a chosen population of spermatozoa.
After this time, if the fertilization took place, as happens in 70-90% of cases, the embryos are transferred to the uterus; generally their number is chosen according to the woman's age: 1-2 if she is under 36, 2-4 in older women. Those remaining, called supernumeraries, are frozen and stored for years.
Embryo conservation
The need to preserve these embryos stems from the fact that repeated ovarian stimulation operations, in addition to being costly in economic terms, can be dangerous for a woman's health. Seen in this light, the freezing of embryos in liquid nitrogen (-196 ° C) represents a precious resource if the first attempts to give birth to a child should fail.
In Italy, however, it is possible to produce no more than three embryos at a time, ie the number needed for a single, contemporary plant. An alternative to embryo freezing, prohibited in our country, could be to do the same with egg cells. This possibility raises a number of much lower ethical problems; unfortunately, however, the biological characteristics of the egg cell make the operation rather delicate and it is still early to assess whether its freezing is completely harmless to the health of the unborn child.
Probability of Success
Of the 2-4 embryos transferred to the woman's uterus, at least one should be able to implant herself and thus establish the long-awaited pregnancy.
The number of embryos is therefore chosen by mediating between the possibility of failure and a possible multiple pregnancy.
This is an important choice because a multiple pregnancy could compromise the pregnancy outcome itself and the health of the mother and fetuses. On the other hand, however, the success rates of in vitro fertilization are not very high, so much so that we speak on average of 35% if the woman is under 36, up to percentages lower than 9% for ultra-quarters. Furthermore, the abortion rate is quite high, close to 20%, as is the risk of twin pregnancies. There also appears to be a greater likelihood of premature births and underweight babies.
Law and Ethical Aspects
The discussed limitations of the Italian law concern above all in vitro fertilization, for which limits were imposed on the number of embryos to be produced, the prohibition of cryopreserving them and the obligation to transfer them all at the same time in utero. This law, deeply disputed by many, but in harmony with the ethical sensitivity of others, is the result of a series of considerations, first of all: what to do with the remaining frozen embryos? Use them for research, since they are a source of stem cells and can assess the teratogenic effects of new drugs, or, more simply, destroy them?
Questions that we deliberately leave open to make room for the reader's sensitivity and morality. Questions to which Italian law - heavily influenced by confessional choices - has given clear answers: no to experimentation with embryos, no to their freezing. These and other limitations, such as the impossibility of performing the pre-implantation diagnosis, for the purpose - for example - of knowing the concrete possibility that the unborn child may have hereditary diseases, represent an insurmountable constraint for many couples.
An obstacle that can be circumvented. turning to structures in other states where regulations are less restrictive. We cannot in fact forget the increasingly numerous couples who go abroad in search of a child who does not arrive here, precisely because of the limitations imposed by this law. A journey of hope, expensive, sometimes too much for the pockets of the partners, but which in many cases is the only way to crown a dream that is priceless, because most of the time it is the result of a love that should at least make us think. whoever does - or at least says he does - has his own reason for living.