Generality
An abdominal aortic aneurysm is a permanent pathological dilation, a sort of bulge similar to a ball, which affects the wall of the largest artery of the abdomen.
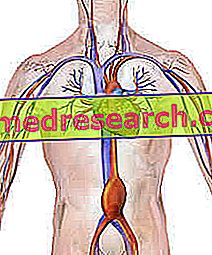
Figure: illustration depicting an aneurysm (swelling) of the abdominal aorta. From the site: wikipedia.org
Although the precise causes are currently unknown, doctors believe that the onset of an abdominal aneurysm is favored by various factors, such as hypertension, aging, cigarette smoking, etc.
Symptoms, when present, consist of a strange pulsating sensation at the level of the navel, accompanied by persistent abdominal pain and lumbar pain.
For a precise diagnosis, in addition to the physical examination, an abdominal ultrasound scan, a CT scan and / or a nuclear magnetic resonance are usually required.
The therapy involves surgery, which is generally practiced only in the case of large aneurysms.
Short recall on aneurysm and aorta
An aneurysm is a pathological dilation of a blood vessel, usually an artery.
The health problems derive from the fact that, once dilated, the vessel wall weakens and can break easily; in case of breakage, the consequent loss of blood can be massive and even lead to death.
Furthermore, even if it does not break down, a large aneurysm can still affect the correct blood circulation and favor the formation of blood clots or thrombi.
The aorta
The aorta is the largest and most important arterial vessel in the human body. It originates directly from the heart (left ventricle) and, thanks to its innumerable branches, spreads the blood towards every anatomical district: head, upper limbs, organs of the abdomen and lower limbs.
On a purely didactic level, the aorta is divided into two main segments: thoracic aorta and abdominal aorta
What's this
An abdominal aortic aneurysm, more simply called an abdominal aneurysm or AAA, is a pathological swelling of a portion of the aorta tract passing through the abdomen.
As with any other aneurysm, the aortic wall affected by the swelling is fragile and can break relatively easily, causing severe blood loss.
To give an idea of the severity of abdominal aneurysms, consider that 70-90% of spontaneous rupture cases end with the death of the affected subject.
Together with cerebral aneurysms, those affecting the abdominal aorta are the aneurysms that most endanger an individual's life.
CLASSIFICATION
- Under normal conditions, in the adult, the diameter of the abdominal aorta measures about 20 millimeters (ie 2 centimeters).
- We speak of an abdominal aneurysm when the aortic swelling reaches at least 30 millimeters (or 3 centimeters) in diameter.
- The aneurysm is considered large when it reaches a diameter of 55 millimeters (5.5 centimeters).
WHERE DO THE ABDOMINAL ANEURISMS LONELY RESIDUE?
Abdominal aneurysms can arise at various points in the abdominal aorta: below, above and at the same level as the kidneys (respectively, the subrenal, suprarenal and pararenal positions), and near the branch leading to the iliac arteries .
According to statistical research, 90% of abdominal aortic aneurysms are subrenal .
Readers should be reminded that the aorta can also be affected by an aneurysm at the thoracic level. In these cases we speak of a thoracic aortic aneurysm .
Epidemiology
The formation of an abdominal aneurysm is much more frequent among people of advanced age (NB: above 65 years, there is a noticeable increase in the number of cases), among smokers and among subjects suffering from hypertension.
Furthermore, it has been noted that men are more affected than women and that the most affected breed is Caucasian.
According to some statistical studies, men over the age of 65 have a 1 to 3% chance of experiencing an AAA breakup.
As mentioned above, mortality in the event of an abdominal aneurysm rupture is very high (between 70 and 90%).
Causes
The precise cause that leads to the formation of an abdominal aortic aneurysm is unknown.
Many doctors and scientists, however, agree in attributing a fundamental role to factors such as:
- Aging . The blood vessel wall is composed of elastin and collagen. The first ensures elasticity to the vessels; the second guarantees its strength and resistance to stress.
It has been established that aging causes a progressive loss of both elastin and collagen; this stiffens and makes the vessel wall more fragile, therefore it is also more easily subject to permanent expansion and breakage.
- Atherosclerosis . It is a degenerative disease that affects medium and large caliber arteries and depends on numerous risk factors (such as smoking, obesity, diabetes, sedentary lifestyle, etc.).
Atherosclerosis is characterized by the accumulation of fat and other substances (so-called atherosclerotic plaques) on the inner wall of vessels; these, once inflamed, can break and cause bleeding. This haemorrhage is followed by the normal coagulation process, which, however, when it occurs inside the vessels and in the vicinity of what remains of the atheromas, can have dangerous consequences: thrombi or blood clots may form, which add up to the atherosclerotic plaque hindering normal blood flow.
- Hypertension . High blood pressure is triggered by numerous factors, including: overweight, obesity, physical inactivity, cigarette smoking, aging, stress, a certain genetic predisposition, hypercholesterolemia, etc. Consequently, all these situations are also factors favoring an abdominal aortic aneurysm.
- Cigarette smoke . Cigarette smoking, both active and passive, in addition to directly damaging the arteries, also promotes the formation of atheromas and the rise in blood pressure.
- Vasculitis . It is the medical term that indicates an inflammation of the blood vessel walls. It can be caused by an infection, an allergy, some types of cancer, some autoimmune diseases or certain drugs.
- A specific genetic predisposition . Individuals who have a family history of abdominal aneurysm are predisposed to develop these disorders more easily and earlier than usual (ie before the age of 65). This has led us to think that the genetic component also plays a fundamental role.
Summary of the main factors favoring the appearance of an abdominal aortic aneurysm:
- Aging
- Hypertension
- Cigarette smoke
- Vasculitis
- Genetic predisposition
- Diabetes
- Hypercholesterolemia
- sedentary
- Obesity
- Male sex
Usually, the factors described above act in concert, ie together. Therefore, it is easier for an individual to develop an aneurysm if he is both a smoker and suffering from hypertension or if he is a smoker, obese, genetically predisposed to the problem and so on.
Symptoms and Complications
To learn more: Symptoms Aortic aneurysm
The abdominal aortic aneurysm is often asymptomatic (that is, devoid of obvious symptoms): according to some statistical surveys, in fact, about 7 out of 10 affected individuals do not show any noteworthy disturbance.
In the remaining cases, in which it is symptomatic, the abdominal aneurysm can cause:
- A strange pulsating sensation at the level of the navel.
- A deep and constant pain inside the abdomen or on one side only (the pain sensation is due to the pressure that the dilation, created by the aneurysm, exerts on the adjacent anatomical structures).
- A pain in the lumbar area.
WHAT ARE ASINTOMATICITY RELATED TO? AND THE PRESENCE OF SYMPTOMS?
Often, the presence or absence of symptoms is linked to the size and growth rate of the abdominal aneurysm. In fact, in fact, asymptomatic aneurysms are small and slow in development, while symptomatic aneurysms are mostly large and fast growing.
WHEN TO REFER TO THE DOCTOR?
If you experience one or more of the above symptoms, it is good practice to contact your doctor. Moreover, if for some reason you are a strongly risky subject, it is equally appropriate to undergo periodic checks ; for example, we recommend a specialist visit to:
- Large smokers, 65 or older
- People aged 65 and over, male and suffering from hypertension
- Smokers with a family history of abdominal aortic aneurysm
- Men with a family history of AAA, suffering from obesity
COMPLICATIONS
Abdominal aortic aneurysms, especially if large, can rupture and cause bleeding so important and consistent that it can even lead to the death of the individual.
The symptoms and signs usually caused by the rupture of an abdominal aneurysm are:
- Intense and persistent abdominal and lumbar pain
- Pain radiating from the lumbar area to the legs
- Intense sweating
- Dizziness
- Nausea and vomit
- Hypotension (ie low blood pressure)
- Fast pulse
- Loss of knowledge
- Breathing difficulties
Another serious consequence, which can take place following an abdominal aneurysm, is the easier formation of emboli within the vascular system.
Emboli are almost always blood clots able to move from the place of origin (in this case the aneurysm) to other contiguous arteries of smaller diameter, located for example in the legs, feet or abdominal organs (kidney, liver etc); once a vessel with a diameter small enough to prevent its advancement is reached, the embolus blocks the flow of local blood like a stopper.
Size of dilation and probability of aneurysm rupture
- 40 mm - 55 mm: the probability of breaking is 1%
- 55 mm - 60 mm: the probability of breaking is 10%
- 60 mm - 69 mm: the probability of breaking is 15%
- 70 mm - 79 mm: the probability of breaking is 35%
- 80 mm or more: the probability of breaking is 50%
Diagnosis
A doctor can notice the presence of an abdominal aneurysm even with a simple physical examination, as, at the phonendoscope, he can hear a particular and completely characteristic noise.
However, in order to delineate the precise characteristics of the aneurysm (size, position, gravity etc.) different diagnostic procedures are required, much more precise, such as abdominal ultrasound, CT and nuclear magnetic resonance.
Attention: the physical examination is reliable in most cases; however, if the abdominal aortic aneurysm is small, the doctor may not hear any indicative noise. Therefore, without further investigation, the problem remains unnoticed.

Figure: probe for performing an abdominal ultrasound. From the site: emergencyultrasound.com
ABDOMINAL ECOGRAPHY
Abdominal ultrasound is an instrumental exam sufficiently comprehensive and free of danger. The survey involves the use of an ultrasound probe, which, once placed on the patient's skin, is able to project the internal organs of the latter onto a monitor.
Where the probe rests, the doctor spreads some gel, which only serves to improve the quality of the images.
In the case of an abdominal aneurysm, ultrasound allows not only to locate the exact point of dilation, but also to measure its diameter.
TAC (OR COMPUTERIZED AXIAL TOMOGRAPHY)
CT ( computerized axial tomography ) provides clear images of the internal organs, minutely showing the appearance of the aorta and of the other arterial vessels that depart from it.

Figure: image obtained by CT scan showing an abdominal aortic aneurysm.
From the site: oakvillevascular.com
It is minimally invasive, as it exposes the patient to a minimal dose of X-rays, which are harmful ionizing radiation.
NUCLEAR MAGNETIC RESONANCE (RMN)
Thanks to the creation of magnetic fields, nuclear magnetic resonance provides a precise image of the organs contained in the abdomen, including the aorta and its first branches.
It is not invasive and does not involve the use of radiation harmful to humans.
Treatment
To learn more: Drugs for the treatment of Aortic Aneurysm
The only way to treat an abdominal aortic aneurysm is to intervene with an ad hoc surgical operation.
However, it must be specified that surgery is reserved only for patients with aneurysms larger than 55 millimeters (5.5 centimeters).
In fact, when the aortic dilation is small, it is preferable to limit oneself to the principle of "watching and waiting" (or principle of "surveillance" ).
WHY IS IT PREFERABLE NOT TO OPERATE THE SMALL DIMENSIONS OF THE ANEURISMS?
The surgical operation for the resolution of an abdominal aneurysm is very delicate and the risk of the patient dying during its execution is concrete. Therefore, it is practiced only when the risk of death due to ruptured aneurysm is greater than the risk of death due to complications related to surgery. In other words, the doctors decide to work only if the presence of the aneurysm is considered more insidious than the operative practice.
As anticipated, the most dangerous abdominal aneurysms are the large ones.
WHAT IS THE PRINCIPLE OF "LOOKING AND WAITING"?
The principle of "watching and waiting" consists in subjecting the patient to an abdominal ultrasound every 6-12 months. According to the doctors, this is a great way to monitor the situation and to notice in time an eventual enlargement of the dilation.
SURGICAL PROCEDURES
To repair the abdominal aorta affected by aneurysm, there are two surgical options:
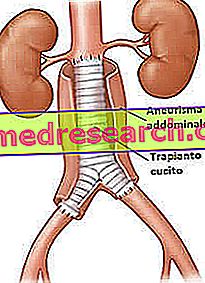
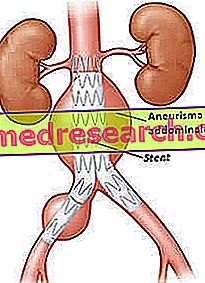
Figure : endovascular procedure. The stent is introduced into the aorta and strengthens the most fragile vascular wall of the normal.
From the site: hackensackumc.org The traditional procedure, or "in the open" .
It consists in removing the aorta section affected by the aneurysm, and then replacing it with a structure of similar shape but made of synthetic material. In other words, the surgeon performs a sort of transplant.
This approach is very invasive, because it involves the incision of the abdomen and an important arterial vessel such as the aorta.
Post-operative recovery can take up to 30 days.
- The endovascular procedure
It consists in reinforcing the walls of the aneurysm by inserting, inside the dilatation, a circular metal prosthesis similar to a net (called stent). The prosthesis is positioned by a catheter inserted into an artery of the leg and led up to the aorta.
Once positioned, the stent is fixed with metal clips, so that it does not move from its position.
The advantage of this procedure is the low invasiveness and the shorter recovery times compared to the traditional technique.
The disadvantage is that the stent could become detached, thus making it necessary to carry out another operation. To ensure that the stent remains in the correct position, it is advisable to carry out an abdominal ultrasound every 6-12 months.


According to a statistical study, the two procedures, if successful, guarantee similar results: the long-term survival rate is in fact overlapping.
What parameters does the choice of surgical procedure depend on?
To choose which procedure is best to adopt, the doctor evaluates the age of the patient, his general state of health (renal function etc.) and the site of the aneurysm.
IN CASE OF BREAKAGE OF AN ABDOMINAL ANEURISM
When an abdominal aortic aneurysm undergoes rupture, it is necessary to intervene immediately, within a few minutes; such a situation is indeed very serious and can lead to death in a very sudden way.
OTHER ADVICE AND PREVENTION
To avoid further deterioration of conditions, in the presence of an abdominal aneurysm the doctor recommends the patient to:
- Not smoking
- Practice physical activity regularly
- Eat healthy and in a balanced way, therefore limit food doses, fatty foods and salt
- Lose weight, in case of overweight and obesity
- Don't drink alcohol
- If you suffer from diabetes, hypercholesterolemia, hypertension, etc., treat yourself according to your doctor's instructions
These same indications also apply to the level of prevention . However, it must be remembered that if there is a genetic predisposition to the formation of aneurysms, even the adoption of the correct preventive measures may not be sufficient to prevent their appearance.
Prognosis
Very often, the individual who develops an abdominal aneurysm is also at risk of the other cardiovascular diseases associated with it ( coronary heart disease, stroke, arteriopathy of the lower limbs etc.). Not surprisingly, most of these patients die from a heart attack or a stroke, while deaths due to ruptured aneurysm are far rarer.
POST-INTERVENTION MORTALITY
Mortality, after a (successful) correction of an AAA, has decreased in recent decades; at the moment (2014), in the Western world its value is equal to 1.6%.
The mortality rate after an operation to remedy the spontaneous rupture of an abdominal aneurysm is clearly higher; in fact it is around 40%.


