Meningococcal
Meningococcus ( Neisseria meningitidis ) is the etiopathological agent involved in meningitis and meningococcal sepsis; in the previous article we presented the pathogen from the microbiological point of view, also focusing on the etiopathogenesis, therefore on the mode of infection. In this article the attention will be directed to the description of the diseases mediated by meningococcus, as well as to the analysis of symptoms and possible therapeutic strategies.
Meningococcal meningitis
The arachnoid and pia mater are the preferential targets of meningococcus: at the leptomeningi level, the bacterium triggers a severe, acute and sudden purulent inflammatory process, which only in some cases resolves itself positively.
Symptoms of meningitis
In infants, meningococcal meningitis manifests itself as an infection of the upper airways which, apparently, is of simple resolution: symptoms can be misleading, causing meningitis to be confused with a slight influence, which can create a diagnostic delay, complicating the prognosis.
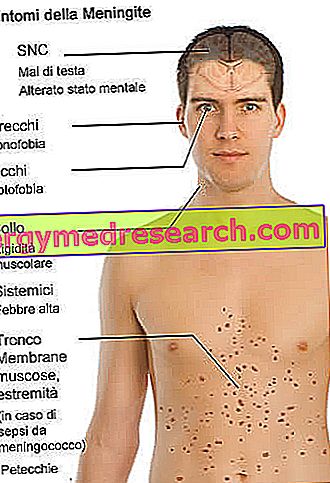
The incubation time for meningococcus is around 24 to 48 hours; after a couple of days from the infection, the symptoms start suddenly, and the victim is hit by psychomotor agitation, alteration of the menstrual cycle (in women of child-bearing age), drop in blood pressure, cervical pain, neck pain, high fever, photophobia, lack of appetite, headache (which in the child is recognized by the so-called "meningeal cry"), stiffness in the neck muscles and vomiting.
It is observed that children affected by meningococcal infections often develop marked mental confusion and convulsions, up to the coma.
In cases of severity, the patient can suddenly develop hemorrhagic skin lesions, ranging from simple petechiae to actual ecchymoses (typical meningococcal meningitis with degeneration in fulminant sepsis).
The symptoms tend to occur in a few hours, up to a few days; not all characteristic signs, however, may develop as a result of meningococcal infection. Consult your doctor immediately in the event of flu-like symptoms that worsen over a few hours or a few days.
Cure of meningitis
Antibiotics and corticosteroids are the drug of choice for the treatment of meningitis: antibiotics remove the pathogen, while steroid derivatives exert their therapeutic action through a marked anti-inflammatory mechanism. The most widely used antibiotic drugs are Benzilpenicillin, Cefotaxima, Rifampicin and Chloramphenicol, while the first choice corticosteroid is dexamethasone. To lighten the symptoms, the patient can take, when necessary, drugs with an anticonvulsant and hypertensive action (in the event of a drop in blood pressure).
The prognosis depends on when the antibiotic therapy is started: obviously, the more you delay the start of the treatment, the more the chances of a poor prognosis increase. When therapy is started late, but the patient manages to survive, the risk of permanent brain damage or deafness increases excessively. WITHOUT PHARMACOLOGICAL THERAPY, THE MENINGOCOCCO KILLS THE GUEST.
Sepsis and septic shock
There is talk of meningococcal sepsis when meningococcus diffuses through the blood into the various anatomical districts: it is estimated that this complication of meningitis affects a tenth of the patients infected with meningococcus (although it sometimes occurs without associating with inflammation of the meninges).
Symptoms
Severe meningococcal sepsis can be fulminant for some patients, but it can also progress with very few and vague signs of meningeal alteration. The vast majority of patients affected by meningococcal sepsis suffer from a high fever (over 39 ° C), associated with a rash with or without hemorrhage: as mentioned above, meningococcal sepsis can develop papules or petechiae, leading to severe ecchymoses, shock and disseminated intravascular coagulation. In addition to these characteristic symptoms, a patient suffering from meningococcal sepsis can also complain of lactic acidosis, headache, hypoperfusion (significant reduction in blood supply to one or more organs), hypotension, myalgia, oliguria and vomiting.
The evolution of meningococcal sepsis is also known as Waterhouse-Friderichsen syndrome or, more simply, fulminant purpura. Mortality, in similar circumstances, is close to 80%, even in the case of early diagnosis.
Treatment of sepsis
When possible, the patient is treated with antibiotics: drug treatment, however, does not always guarantee a good prognosis. Patients who have reached the severe stage of meningococcal sepsis need medical monitoring in the intensive care unit, associated with assisted ventilation and intubation to facilitate respiratory movements as much as possible. Even steroid drugs can sometimes relieve inflammation. For further information: read the article on drugs for the treatment of sepsis.
Prevention
The Prevention Services must respond with immediate urgency in the event of reporting a clinical suspicion of meningococcal meningitis: in such circumstances, a plan for prophylaxis must be promptly implemented. All those who are exposed (or have been) with a high risk of meningococcal infection (for example, the relatives of an affected patient) must undergo chemoprophylaxis; please note that the risk of infection is extremely high in the first few days after the onset of the infection symptoms.
Chemoprophylaxis, carried out within 48 hours of contact with the infected person, consists of the administration of Rifampicin, ceftriazone and ciprofloxacin.
As regards vaccination with preventive purposes, antimeningococcal vaccine for children (conjugated vaccine for meningococcus type C) is available on the market, which ensures long-term protection exclusively against type C meningococcus.
What changes since 2017
With the decree law on the prevention of vaccination for minors from zero to 16 years, approved on 07/28/2017 the vaccine against meningitis ( Haemophilus Influenzae type b vaccine) has become mandatory for those born since 2001 .
As far as vaccinations against meningococcus C and meningococcus B are concerned, although they are not mandatory, they are offered by the Regions and Autonomous Provinces, based on the indications of the vaccination calendar for the year of birth:
- those born between 2012 and 2016 are offered free antimeningococcal vaccinations C
- those born in 2017 are offered free antimeningococcal B, anti-meningococcal C and pneumococcal vaccinations
For more information on mandatory vaccines in children, see this article.


