"An injured and unstable ankle is the prerequisite for recurrent distortions, so we understand the importance of a good re-education after a distortion episode"
In Italy, an estimated 5000 ankle sprains per day are estimated, which means that it is one of the most common traumas in sports and recreational activities.
The ankle sprain is the most frequent musculoskeletal trauma of the lower limb. The sports where this trauma is more frequent, in ascending order, are: volleyball (56%), basketball (55%), soccer (51%) and endurance race (40%).
In the ankle sprain almost always remains a significant enough residual pain that involves a functional limitation. Even after the trauma has been treated there is a variable percentage of patients, ranging from 10% to 30%, who complain of chronic symptoms characterized by synovitis, tendinopathy, rigidity, increase in volume, pain and muscle insufficiency, associated or not to instability of the instep with difficulty in ambulating on uneven terrain or recurrent distortion episodes, regardless of the treatment of the acute episode. This happens because the damage of the distortive trauma does not only occur in the ligamentous tissue, but also in the nervous and muscle-tendon tissue, around the ankle complex.
The time required for complete functional recovery, whatever the treatment reserved for the patient (surgical or conservative), varies from 3 to 5 weeks; the time required before returning to work varies from 4 to 7 weeks; and before the patient can return to sports, it takes 10 weeks. Recovery times are usually shorter in professional athletes because the time reserved for rehabilitation is much longer than for example for an amateur sportsman.
Distortive traumas can be acute (following bumps, contrasts, fights or sudden changes of direction) or chronic (after considerable and prolonged loads).
Distortion is the momentary and incomplete loss of articular relationships between two bony heads.

To learn more: Anatomy and Functions of the Ankle
The traumatic event can lead, in an athlete's ankle, to an articular pathology, divided into two sections:
- that of laxity, with capsular lesions, distension and lacerations of the lateral and medial ligamentous compartment of the ankle and subtalus, which determine an articular excursion beyond the physiological limits;
- that of instability, which the athlete perceives as a sign of joint failure during the sporting and anatomopathologically objectivable gesture in a more or less total rupture of the ligaments.
Size of the Problem:
- 5000 sprains every day in Italy
- 20% sports injuries
- chronic dysfunction in 30% of cases and frequent relapses
- high social costs
"An injured and unstable ankle is the prerequisite for recurrent distortions, so we understand the importance of a good re-education after a distortion episode"
Classification
- Grade 0: astragalus tilt less than 8 °, not ligament tears;
- Grade 1: astragaltic tilt (10 ° -20 °), anterior peroneal-talar ligament rupture;
- Grade 2: astragaltic tilt (20 ° -30 °), rupture peroneal-anterior talar ligament and calcaneal peroneus;
- Grade 3: astragaltic tilt greater than 30 °, rupture of three ligaments
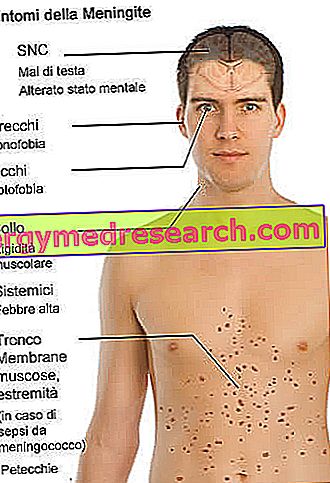
Symptoms
To learn more: Ankle Sprain Symptoms
- Live pain, located in the anterior area of the peroneal malleolus, which occurs during palpation;
- Modest or conspicuous swelling at the periarticular and articular level, a sign of the rupture of the small passing arteriola above the anterior peroneal-talar ligament (sign of Robert-Jaspert);
- Functional limitation caused by the pain that the patient feels during the movements of the joint;
- Tibial-tarsal articulation instability
Conservative treatment
To learn more: Remedies for Ankle Sprain
It is divided into 3 phases : Acute Sub-acute of Functional Re-education
ACUTE PHASE
The most accredited protocol for acute injuries is the PRICE Protection Rest Ice Compression Elevation In the acute phase the objectives are: a) Immobilization; b) Decrease of "chemical irritants" that cause pain and favor "tissue stasis" (or edema); c) Prevention of further mechanical stresses of the injured structure.
SUBACUTE PHASE
In the subacute phase, the purpose of the treatment is to subject the damaged tissue to a series of mechanical stresses, useful for promoting the physiological orientation of the collagen fibers. The objectives in this phase are: a) The elimination of pain; b) The recovery of particularity; c) The elimination of muscle spasm; d) Elimination of the edema; e) Recovery of muscle strength. To achieve these goals, massages, physical therapies, mobilization techniques and kinesitherapy are used.
FUNCTIONAL RE-EDUCATION PHASE
In the functional re-education phase, the aim is: a) Recovery of proprioception; b) Recovery of strength; c) Prevention of recurrences.
THE FUNCTIONAL BANDAGE prevents the onset of relapses or relapses when physical activity is resumed; avoids the damages of a prolonged immobilization or functional inactivity; reduces recovery time
If an ankle sprain occurs in adverse places, far from possible rescue, it is best not to remove the shoe to examine the lesion. The resulting pain associated with swelling could in fact hinder the reintegration of the foot into the shoe.
CONTINUE: Sprained ankle: proprioceptive and muscle strengthening exercises »